Protecting Independent Medical Practice Revenue Through Accurate Taxonomy Mapping
Most independent practice leaders focus heavily on provider credentialing, payer enrollment, and the signing of insurance contracts when spinning up a practice or expanding service lines. Taxonomy codes often receive far less attention during this phase, despite being one of the foundational validation data points insurers use to determine whether a provider should be reimbursed for a service in the first place.
Operational Snapshot
Taxonomy codes function as a foundational reimbursement control point, even though they receive far less attention than credentialing and payer enrollment. When left unchecked, they can quietly create claim denials, aging A/R, and downstream revenue cycle disruption.
Because taxonomy codes operate in the background of most practice management and EHR billing systems, many practices do not review them until denials begin appearing. By that point, the issue is no longer a simple administrative oversight. It becomes an immediate revenue-cycle bottleneck, causing aged accounts receivable (A/R). It undermines opportunities for network participation and strains relationships with commercial payers.
Understanding how taxonomy codes interact with credentialing, payer enrollment, and insurance contracting can help practices reduce preventable denials and streamline the claim submission process.
Key Takeaways
- Taxonomy codes influence reimbursement eligibility and claim adjudication.
- Payers use taxonomy data during credentialing and network participation decisions.
- CPT-to-taxonomy mismatches can trigger automated denials.
- Behavioral health and specialty practices face elevated taxonomy-related risks.
- NPI Type 1 and Type 2 taxonomy alignment requires ongoing oversight.
- Taxonomy reviews should be incorporated into routine revenue cycle audits.
Table of Contents
What Taxonomy Codes Actually Do: A Deeper Operational Look
A healthcare provider taxonomy code is a unique, standardized alphanumeric identifier used to define a provider’s type, classification, and precise area of specialization. Providers elect these codes during the initial application for their National Provider Identifier (NPI) via the National Plan and Provider Enumeration System (NPPES).
This profile selection becomes part of the provider’s NPPES record and should be maintained as the provider’s credentials, services, or practice setting change. Insurance clearinghouses and payers may use this information alongside credentialing, enrollment, roster, and contract data to evaluate whether billed services align with the provider’s profile.
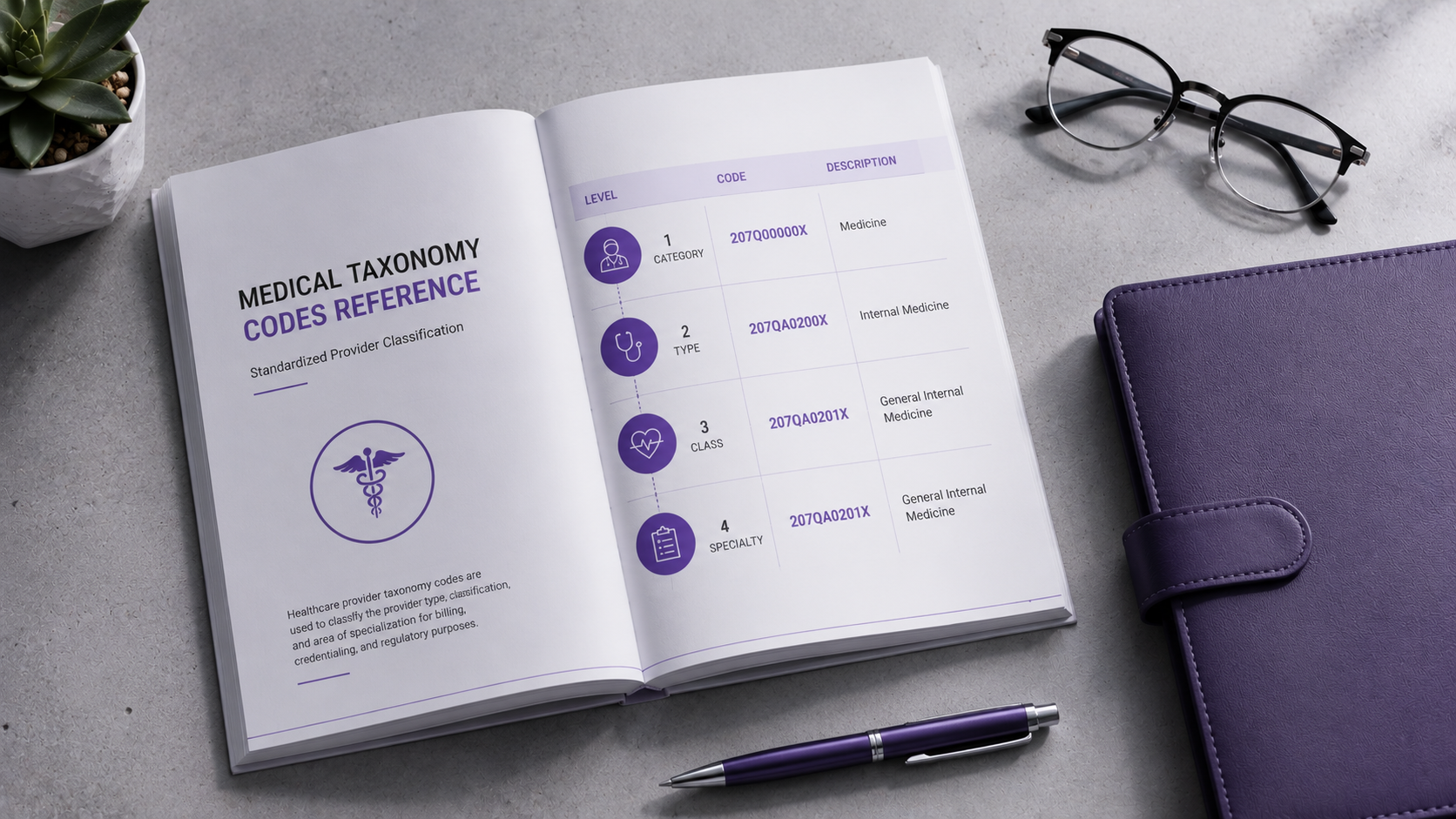
At its core, a taxonomy code is a 10-digit character string that always ends with the letter “X.” The National Uniform Claim Committee (NUCC) deliberately structures this code into three distinct parts to communicate specific operational criteria:
- Provider Grouping (Characters 1–2): Establishes the broad, high-level provider category, distinguishing between major medical branches such as Allopathic Physicians, Osteopathic Physicians, Physical Therapists, or specialized clinical technicians.
- Classification (Characters 3–6): Identifies the general medical specialty focus or clinical department, such as Family Medicine, Pediatrics, or Internal Medicine.
- Area of Specialization (Characters 7–10): Pinpoints the precise clinical subspecialty or niche focus within that broader classification (e.g., Pediatric Neurology or Pediatric Endocrinology). The final character “X” serves as a uniform structural placeholder required by EDI (Electronic Data Interchange) clearinghouses to meet standard 10-digit processing lengths.
In many taxonomy codes, the final “X” functions as part of the standardized code structure.
This structure allows adjudication systems to distinguish between providers who share a broad specialty classification but practice in different clinical environments. From an operations standpoint, taxonomy codes are the mechanism that tells an insurer whether the services being billed align perfectly with the provider’s recognized area of practice.
Are you struggling with mysterious claim denials? Sometimes the root cause isn’t your coding or documentation. It’s the taxonomy codes on your NPI profile. In my latest video, I break down exactly what these codes are, how they impact your reimbursements, and provide a quick, step-by-step guide to verifying your practice’s NPI 1 and NPI 2 taxonomy records to keep your billing on track.
The Anatomy of an Algorithmic Claim Denial
When an 837P professional or 837I institutional electronic claim file hits an insurance carrier’s processing engine, the system is running a series of rapid, automated gatekeeping validation checks. Before a human claim processor ever reviews the medical necessity or documentation of a claim, the payer’s adjudication engine cross-references the data fields using strict logic:
- Affiliation Check: Is the rendering provider’s individual NPI (Type 1) actively mapped and associated with the billing group’s organizational NPI (Type 2)?
- Roster Check: Is the rendering provider actively credentialed, contracted, and loaded onto the group’s active insurance roster for this specific plan?
- Scope & Code Check: Does the submitted CPT (Current Procedural Terminology) code sit within the approved clinical boundaries of the provider’s self-identified taxonomy code on file in NPPES?
If the payer’s validation process identifies a mismatch, the claim may be rejected, denied, pending for review, or require manual intervention, depending on the payer’s internal editing rules.
Compliance Alert
Some payer adjudication systems compare CPT codes, specialty setup, credentialing data, taxonomy information, and provider roster records before medical necessity is reviewed. A mismatch can trigger an immediate scope-of-practice denial regardless of credentialing status.
This is where growing practices frequently encounter unexpected revenue cycle disruptions. A physician may be fully credentialed and actively treating patients, yet a payer may suddenly deny an entire batch of specialized procedures because the taxonomy code associated with that provider does not support reimbursement for those specific codes under the payer’s internal guidelines.
While manual appeals, peer-to-peer reviews, and clinical documentation submissions can sometimes overturn these denials, certain payers maintain hard-coded policies. These policies require either a completely different specialty designation or a specific subspecialty board certification on file before payment is released. This can create administrative strain, increase days in A/R, and lead to preventable write-offs.
High-Risk Verticals: Where Specialty Practices Intersect with Taxonomy Pitfalls
For standard family practice or general internal medicine clinics, taxonomy-related claim denials may be less common when billed services align with the provider’s general specialty profile. This is because the broad E/M (Evaluation and Management) codes and basic wellness procedures they bill naturally align with general physician classifications and standard Place of Service (POS) 11 guidelines.
However, the compliance and financial risk increase exponentially as a practice increases its clinical specialization. Behavioral health operations are among the highest-risk areas for taxonomy-driven denials.
Compliance Alert
Behavioral health organizations face elevated denial risk because multiple provider types often deliver similar services under one roof. Taxonomy alignment becomes critical when payers restrict psychiatric and diagnostic CPT codes to specific provider classifications.
Within a multi-disciplinary behavioral health setting, multiple provider types—such as Licensed Clinical Professional Counselors (LCPCs), Licensed Clinical Social Workers (LCSWs), Clinical Psychologists, and Psychiatrists (MD/DO)—frequently deliver overlapping clinical services under one roof. However, payers restrict specific psychiatric CPT codes to specific provider classifications.
If an internal medical billing team accidentally applies a highly specialized code (such as a medication management modifier or an advanced diagnostic evaluation code) to a claim where the rendering provider’s NPI is tied to a standard counseling or social work taxonomy, the clearinghouse engine will reject or deny the claim immediately.
For practice leaders, this may appear to be a credentialing issue when the root cause is actually a mismatch in CPT-to-taxonomy, provider roster, or payer specialty setup. Similar patterns occur regularly across surgical subspecialties, advanced occupational health networks, and multi-specialty medical groups.
NPI Type 1 vs. NPI Type 2: Complex Organizational Mapping
Proactive taxonomy management becomes critical as a healthcare business scales out of a solo-provider setup and into a group clinic structure. Clinical operations leaders must manage taxonomy codes across two distinct tiers of National Provider Identifiers:
- NPI Type 1 (Individual): Assigned to an individual clinician, following them across states and employers for the entirety of their medical career. It must accurately reflect their personal training and board certifications.
- NPI Type 2 (Organizational/Group): Assigned to the corporate business entity, clinic group, or healthcare institution for billing purposes.
A common operational misconception is that the group’s organizational taxonomy must exactly match the individual taxonomy codes of every rendering provider. In practice, they simply need to align logically. Understanding the operational relationship between individual and organizational NPIs is critical, particularly as practices expand and onboard additional providers.
For a deeper look at how these identifiers interact within payer enrollment and claims processing workflows, see our guide on NPI Type 1 vs. NPI Type 2 provider data alignment. For example, a multi-specialty medical group does not need to continuously alter or load dozens of highly specific individual taxonomies onto their group NPI. Instead, the National Uniform Claim Committee (NUCC) provides a specific Multi-Specialty Group taxonomy code (193200000X) specifically for organizational NPI Type 2 profiles.
Technical Deep Dive
Multi-specialty organizations do not need exact taxonomy duplication across every provider and group profile. Using the designated Multi-Specialty Group taxonomy creates a contracting umbrella while allowing individual clinicians to maintain specialized Type 1 classifications.
This specific organizational designation establishes a clean corporate contract umbrella with insurance networks, allowing individual clinicians to seamlessly map their highly specialized Type 1 taxonomies underneath the business entity:
[ NPI Type 2: Group NPI ]
(Multi-Specialty Group Taxonomy: 193200000X)
│
┌─────────────────────┼─────────────────────┐
▼ ▼ ▼
[ NPI Type 1 ] [ NPI Type 1 ] [ NPI Type 1 ]
(Behavioral Health) (General Practice) (Allergist)
As practice models evolve, modern medical billing systems enable practices to dynamically map taxonomy information across different payer contracts. This mapping creates flexibility when different payers and clearinghouses roster your group. However, it demands careful operational oversight to prevent downstream accounting glitches.
The Strategic Impact on Contracting: Geographic Payer Panels
Taxonomy codes influence more than claim adjudication; they can also affect how payers classify your practice during credentialing, contracting, and network participation reviews. Insurance networks use macro-level taxonomy data to continuously evaluate their geographic network capacity, monitor provider-to-member ratios, and make structural contracting decisions.
Operational Snapshot
Taxonomy data influences more than reimbursement—it also affects network access and panel availability. Outdated specialty designations can cause providers to be evaluated against the wrong market capacity metrics during contracting.
When an expanding practice or new provider receives a notice that the network panel is closed for a specialty in a specific area, the decision may be influenced by taxonomy data, payer specialty categories, geography, network adequacy standards, and internal provider capacity metrics.
If a provider’s taxonomy is outdated, overly broad, or incorrectly configured as a generic internal medicine profile, they may find themselves locked out of a market panel that actually has active openings for their true niche. This can happen when the provider practices a subspecialty that is not reflected accurately in payer records. Keeping this data current ensures your practice is measured against the correct regional network metrics.
Case Study: Urgent Care, Place of Service 20, and Global Fee Traps
Urgent care clinic operations perfectly illustrate how specialty designation directly affects contractual revenue strategy. Although an urgent care facility operates in an office-based setting, payers treat it as a distinct medical model due to its unscheduled walk-in framework, extended operating hours, and higher ancillary testing overhead. Consequently, urgent care centers must bill under Place of Service 20 (Urgent Care Facility), rather than the traditional Place of Service 11 (Physician Office).
While billing under POS 20 may support different reimbursement considerations than a traditional office setting, it can also introduce contracting terms that practice leaders should review carefully before signing.
If an organization enters commercial contract discussions without a clearly defined specialty classification, matching taxonomy profiles, and a documented ancillary service strategy, it may be more vulnerable to bundled reimbursement terms that limit separate payment for labs, imaging, or other add-on services. As a standard practice management rule, you must analyze your pro forma metrics and explicitly negotiate these clauses. “The proposed global S-code will cover the base evaluation visit, but our contract must include the right to carve out and receive separate, unbundled reimbursement for all ancillary laboratory and imaging items.” In high-overhead environments, taxonomy data is a vital lever for revenue optimization.
Data Governance: The Mechanics of Adding vs. Removing Taxonomy Codes
The National Uniform Claim Committee database publishes its official taxonomy options updates twice a year to reflect shifts in the clinical landscape. When a clinic’s operational profile or service lines change, but its taxonomy data remains static, backend reimbursement issues may arise. Practices should implement a biannual audit of both their individual and organizational NPI profiles within the NPPES portal. However, updating this data requires strict adherence to operational safety protocols:
- Adding or Correcting Codes (Low Risk): This is an easy administrative adjustment. Adding a secondary or corrected taxonomy code to your NPI profile expands your billing footprint and opens up new CPT pathways. It rarely disrupts active cash flow. Individual providers can safely hold multiple distinct codes if they maintain multiple board certifications or cross-functional subspecialties.
- Removing Existing Codes (High Risk — Revenue Warning): This operational step requires extreme caution. If an internal team member removes a taxonomy code that is still tied to payer credentialing records, active claims may be rejected or denied, or require manual correction until payer files are updated. This can create preventable claim delays until payer and clearinghouse records are reconciled.
Compliance Alert
Adding taxonomy codes is typically low risk, but removing active codes can interrupt claims processing if payer records have not been updated. Always reconcile insurance rosters and credentialing files before making deletions in NPPES.
Never purge an established taxonomy code from the national database without first verifying that your regional payer contracts have been updated to match the new operational structure. A comprehensive review of your taxonomy profile should occur before:
- Initiating applications for new commercial or government insurance contracts.
- Beginning the credentialing process with additional insurance networks.
- Launching new internal service lines, ancillary procedures, or in-house lab testing that may require a CLIA Certificate of Waiver.
- Adding incoming mid-level or specialized providers with distinct training backgrounds.
Final Takeaway: Protecting Your Cash Flow
Taxonomy codes are far more than a minor administrative formality; they are the baseline data points that define how major insurance engines view, categorize, and pay your practice. They may influence automated claim edits, credentialing records, payer roster setup, network participation reviews, and certain contract or fee schedule decisions.
When taxonomy information is inaccurate or outdated, practices often experience claim denials, delayed reimbursement, and avoidable administrative rework. Assign a specific individual on your practice operations team to audit these codes twice a year, in conjunction with national database updates. Maintaining accurate taxonomy mapping is one of the simplest ways to protect revenue cycle performance and reduce avoidable cash-flow disruptions.
Common Questions About Taxonomy Codes and Reimbursement
How long does it take for a payer to recognize an updated taxonomy code?
While updates published in the NPPES database populate the registry almost immediately, commercial and government payers can take anywhere from 30 to 90 days to sync this data into their internal adjudication engines. Claims submitted using a new taxonomy before the payer’s system updates are often automatically rejected.
Can a medical practice dynamically map multiple taxonomy codes to different payers?
Yes. Modern practice management and EHR billing platforms allow you to configure taxonomy overrides at the insurance plan level. This enables a provider to submit an institutional claim using a broad group taxonomy to one commercial payer while billing a highly specific subspecialty taxonomy code to another.
What is the safest way to reconcile an incorrect taxonomy code without disrupting cash flow?
Never delete the old taxonomy code first. Instead, submit the corrected or secondary taxonomy code via the NPPES portal, wait for confirmation, and notify your major payer networks to update their internal provider rosters. Request the absolute removal of the legacy code only after your billing team confirms that claims are successfully being adjudicated under the new code profile.
Will an individual taxonomy change require a full contract re-negotiation?
Typically, no. Updating an individual Type 1 taxonomy code is treated as an administrative credentialing demographic update rather than a structural contract alteration. However, changing a group NPI Type 2 organizational taxonomy classification can fundamentally shift your baseline fee schedule or trigger a comprehensive contract amendment review.
How do taxonomy code mismatches impact secondary and tertiary insurance claims?
If the primary insurance processes a claim successfully under a broad specialty classification, a secondary or tertiary payer with stricter automated scope-of-practice edits may still deny its portion of the coordination of benefits (COB) if the provider’s registry taxonomy doesn’t match its exact subspecialty rule.
What specific events should trigger an immediate out-of-cycle taxonomy audit?
Beyond your biannual routine schedule, an immediate audit should occur when launching a cross-functional service line (such as a CLIA-waived laboratory), converting a solo practice into a multi-specialty group entity, or adding mid-level providers (NPs/PAs) whose state-mandated collaborative practice scopes differ from your existing clinical team.
About the Author
Jennifer Blevens-Smith is the founder and sole consultant driving Integral Clinic Solutions. Armed with deep domain expertise and a commitment to protecting independent medicine, she delivers the personalized, executive-level guidance that healthcare leaders need to build sustainable, high-performing organizations.
Need Help Strengthening Your Medical Practice Operations?
Integral Clinic Solutions provides practical support for medical practices navigating credentialing, contracting, revenue cycle operations, compliance workflows, front-office systems, and practice management challenges.
Explore more operational guidance, compliance insights, and healthcare business resources on the Integral Clinic Solutions blog. New articles and updates are added regularly for practice owners, administrators, and healthcare teams.
Disclaimer: This content is for informational and educational purposes only and does not constitute legal, coding, billing, compliance, financial, or medical advice. Healthcare practices must verify all operational requirements with applicable payers, regulators, and qualified professionals. Read our full Legal & Compliance Disclaimer.